A practice can grow its caseload and lose ground on retention at the same time. New patients come in while existing ones quietly disengage and don’t come back.
When that happens, the first instinct is to look at the clinical side. Are patients getting results? Is care consistent across clinicians? Those questions matter, but they’re usually not where the answer lives.
In a growing practice, retention tends to slip for structural reasons. The team is bigger. The owner is less visible. Handoffs that once happened naturally now happen inconsistently, or not at all. Nobody has clear ownership over whether patients actually finish what they started.
What growth does to retention
When a practice is small, retention takes care of itself in a way. The owner treats most of the patients. Relationships are direct. If someone starts falling off, the owner notices. There’s no gap between the clinical experience and the operational follow-through because the same person is managing both.
That changes as the team grows. More clinicians means more variation in how patients experience the practice. More patients means nobody has a complete picture of who’s on track and who isn’t. The owner steps back from the schedule and the relational continuity that once held patients goes with them, unless something deliberate replaces it.
This is the part that catches owners off guard. Retention didn’t slip because care quality dropped. It slipped because the structure that was quietly supporting it no longer works at the new size.
MedBridge research puts the scope of the problem in concrete terms: seven out of ten patients don’t complete all authorized visits. That figure holds across a range of outpatient settings. The practices that beat it aren’t the ones with better clinicians. They’re the ones with better structure around the clinical work.
Four places retention slips
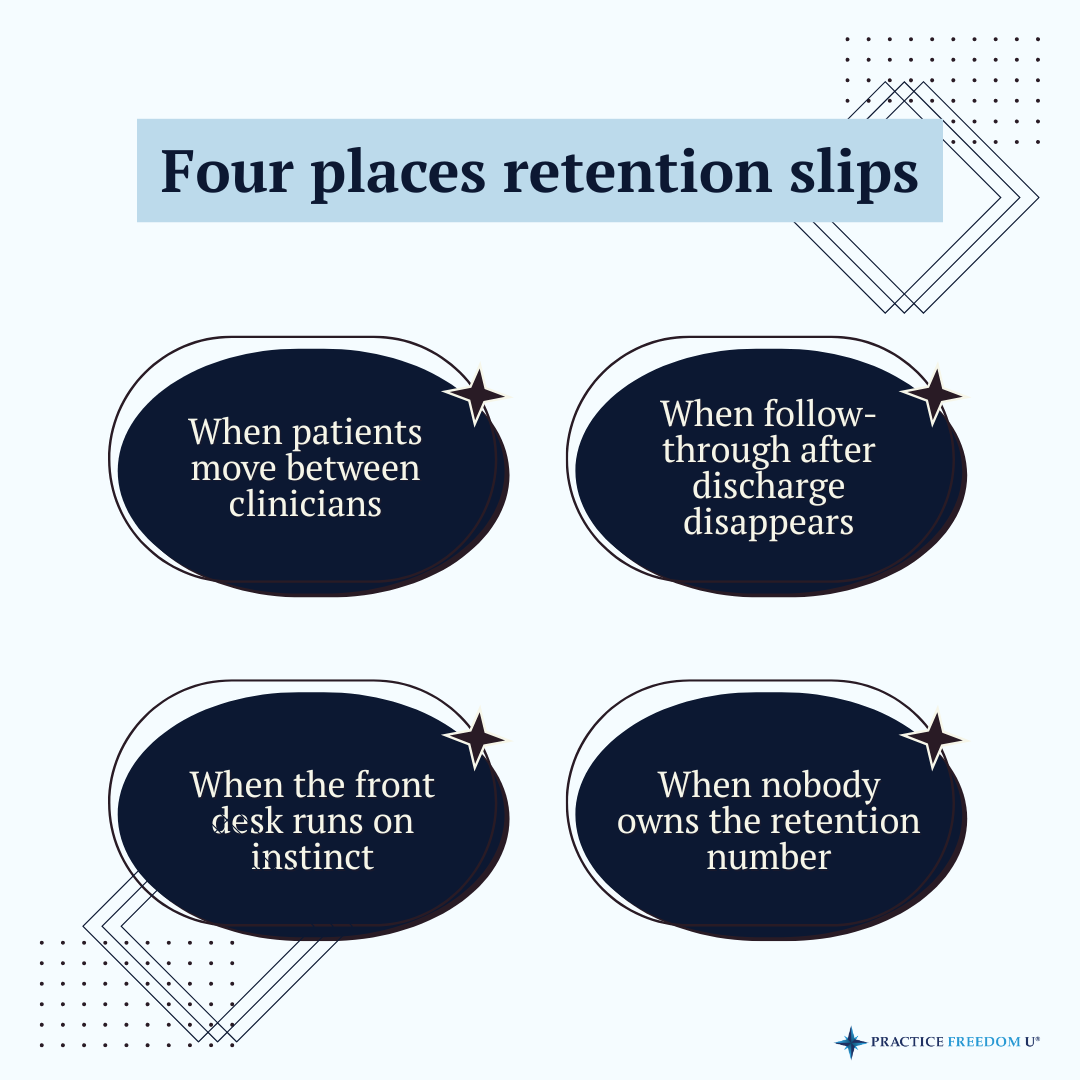
When patients move between clinicians
The relationship a patient has with their original clinician matters more than owners typically account for. When a patient gets transferred to someone new, whether because of scheduling changes, caseload shifts, or the owner stepping back from direct care, and that transition isn’t managed deliberately, the patient’s commitment often goes with it.
A handoff that feels abrupt or unexplained creates doubt. The patient starts wondering whether finishing really matters, whether this new person understands their situation, whether the effort is worth it. Few patients say any of this out loud. They just stop scheduling.
The fix isn’t keeping patients with the same clinician indefinitely. It’s building a handoff process where the transition feels intentional, the new clinician already knows the patient’s history, and the patient understands why the change is happening and what to expect next.
When follow-through after discharge disappears
Discharge is one of the higher drop-off points in a growing practice, and it’s almost never tracked. A patient finishes their plan of care, leaves with a home exercise program, and that’s the last contact the practice has with them.
No follow-up call at two weeks. No check-in at 30 days. No structured way to stay connected. The patient gets on with their life, the original issue returns or a new one surfaces, and they call somewhere else because the first practice didn’t stay in contact.
Practices that retain patients over time have a post-discharge rhythm. It doesn’t have to be elaborate. A call, a brief check-in, a simple touchpoint that signals the practice is still paying attention. What matters is that it happens on a consistent schedule and someone owns the outcome.
When the front desk runs on instinct
The front desk sits at the center of patient retention. In a growing practice, it’s also often the least structured part of the operation. Scheduling decisions get made based on who’s available. Cancellations get followed up when someone has time. Patients who go quiet don’t trigger a consistent response.
None of that reflects poorly on the front desk team. It reflects what they’ve been given to work with. When the expectation is “keep the schedule full” with no defined process behind it, instinct fills the gap, and instinct produces inconsistent results at scale.
A front desk team that can genuinely protect retention needs clear protocols: how to respond to a cancellation, when to follow up and with what, which patients are considered at risk, and what to say when reaching out to someone who’s gone quiet.
When nobody owns the retention number
This tends to be underneath the other three. In a growing practice, patient retention is everybody’s general concern and nobody’s specific responsibility. The owner cares about it. The clinicians care about it. The front desk cares about it. Ask who is accountable for the retention rate this month and there will be a pause.
Diffuse accountability produces slow change. Problems get noticed, surface in team meetings, and persist because no single person’s job is to track the number and move it.
What this costs the practice
Patient retention doesn’t get the same attention as new patient volume because it’s slower to show up in the numbers. Marketing generates leads. The phone rings. The schedule fills. Retention is quieter.
Healthcare research consistently shows that acquiring a new patient costs significantly more than retaining an existing one, with some estimates putting the gap at five to seven times higher. Losing a patient two or three sessions early, across a practice with several clinicians running full caseloads, adds up to a revenue gap that compounds quietly across the year.
Practices that stabilize revenue as they grow aren’t always the ones with the strongest new patient pipeline. They’re often the ones that stop leaking existing patients while filling new ones in. APTA’s own data points to how operational friction, not clinical quality, is frequently what pushes patients to disengage or abandon treatment entirely.
The structural fix
Retention problems in a growing practice don’t get solved by asking clinicians to build stronger relationships or the front desk to try harder. Those conversations happen and the numbers don’t move because the structure underneath hasn’t changed.
Building that structure means four things:
- A handoff process every clinician follows when patients transfer, with language and timing defined
- A post-discharge follow-up rhythm with a clear owner and a consistent schedule
- Front desk protocols specific enough that retention doesn’t depend on individual judgment calls
- A retention metric that gets reviewed on a regular cadence, with one person accountable for the result
None of these require a major overhaul. They require a decision that retention is important enough to build deliberately, rather than assuming the team will figure it out as the practice grows.
Retention slipping as a practice scales is common. It’s also fixable. The patients are often there. The team is capable. What’s typically missing is the system that makes consistent follow-through the default.
Structural problems need structural answers. The practices that figure that out early stop spending on acquisition to replace patients they should have kept.
For more conversations on building the structure underneath a growing practice, listen to Freedom By Design on Apple Podcasts, Spotify, or YouTube.
————————————————————-
Are you ready for a coach? Join the hundreds of physical therapy owners who are building the practice of their dreams with the support, guidance and direction of a Practice Freedom U Coach. Take the first step towards creating a business that sets you free by scheduling a Discovery Call